





Patients with lung cancer treated with epidermal growth factor receptor (EGFR) inhibitors may have an increased risk of new-onset keratitis, a U.S. population-based cohort study showed.
Over a 20-year period, 1.12% of patients who were treated with EGFR inhibitors developed new-onset keratitis compared with 0.74% of those who did not take these drugs (HR 1.520, 95% CI 1.339-1.725), reported Kevin Sheng-Kai Ma, DDS, of Harvard T.H. Chan School of Public Health in Boston, and colleagues in JAMA Ophthalmology.
Specifically, patients treated with EGFR inhibitors — including gefitinib (Iressa), erlotinib (Tarceva), afatinib (Gilotrif), and osimertinib (Tagrisso) — had higher risks of keratoconjunctivitis (HR 1.367, 95% CI 1.158-1.615), superficial keratitis (HR 1.635, 95% CI 1.306-2.047), and corneal ulcer (HR 2.132, 95% CI 1.515-3.002).
Notably, patients taking the second-generation EGFR inhibitor afatinib had the highest risk of keratitis (HR 2.229, 95% CI 1.480-3.356), though the risk was still observed with osimertinib, the standard first-line option in the metastatic setting (HR 1.591, 95% CI 1.130-2.239).
Ma told MedPage Today that clinicians should keep in mind that the drugs can significantly improve the overall survival of lung cancer patients. The findings “don’t tell us to stop EGFR inhibitors,” he said, “but would guide our clinical decisions in terms of whether or not we should follow the patients more frequently if the patients have shown early signs of severe forms of keratitis.”
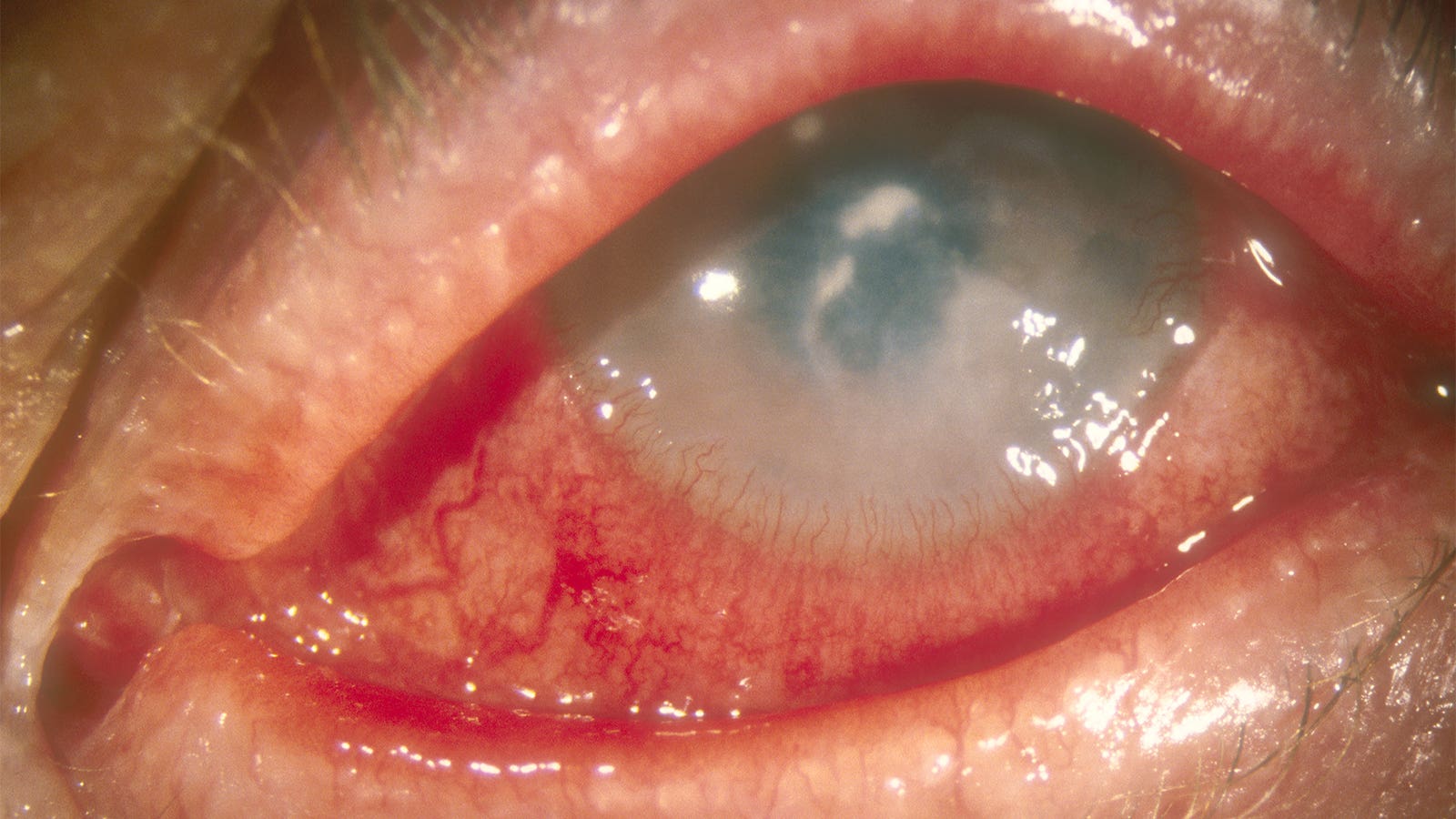
According to the Cleveland Clinic, contact lenses are a major risk factor for keratitis, and other risk factors include weakened immunity and long-term use of corticosteroids. Eye drops are initially prescribed, and corneal transplants may be needed in the most severe cases.
Jeanine Baqai, MD, of Northwestern University Feinberg School of Medicine in Chicago, told MedPage Today that eye doctors see keratitis often.
“It is important to decipher if the cause of this inflammation is infectious or non-infectious,” she said. “If there is concern for infection, we will typically culture the patient and start them on antimicrobial treatment. The infection may be bacterial, viral, fungal, or parasitic. If the inflammation is not felt to be infectious and there is no ulceration, we may treat with steroids. We are fortunate to be able to resolve most keratitis with topical treatment.”
EGFR inhibitors are used to treat several kinds of cancers including lung, breast, colorectal, and pancreatic cancer. Case reports and series have reported ocular adverse effects in patients taking the drugs for lung cancer, Ma noted, but no comprehensive studies have looked at the overall risk or stratified the results by type of drug and type of keratitis.
There are three generations of the drugs available, Ma said, and a fourth is under development. The risk remained steady over the 20-year period of the study, suggesting that the evolution of the drugs over time has not changed the risk level.
The drugs may boost the risk of keratitis by inhibiting healing within the cornea, Ma explained. “All patients taking all those drugs should be instructed by their ophthalmologist, medical oncologist, or primary care physicians about the potential complications from EGFR-targeted therapies.”
Baqai said the link between the drugs and keratitis “is certainly known amongst cornea subspecialists, but it is not a complication we typically see on a regular basis like other conditions.” However, “as more drugs surface, the prevalence with which we see these patients increases.”
“Cancer patients and patients receiving these medications should be examined and evaluated with a very discerning eye,” she added. “Sometimes we can see side effects from medications and other times we can see manifestations related to the cancer itself. It is important to be very thoughtful about the cause and the treatment of any keratitis, since the condition can lead to loss of vision. Expedited referral to the appropriate subspecialist is always recommended.”
For this study, Ma and team examined data from the TriNetX database on 1,388,108 adult patients who were treated for lung cancer from May 2003 through October 2023. The index dates were the date of first prescription for the patients who took the EGFR inhibitors or the date of diagnosis with lung cancer for the patients who did not take these drugs.
Of the total patients, 22,225 received EGFR inhibitors. Mean age was 69.7, and 62.8% were women. About half of patients in both groups had hypertensive diseases; those taking EGFR inhibitors were more likely to have secondary malignant neoplasms.
What’s next? Ma said his team is working on follow-up studies to examine the risk of keratitis by ethnicity, since research has linked ethnic background to EGFR mutation status.
![author['full_name']](https://clf1.medpagetoday.com/media/images/author/RDotinga_188.jpg)
Randy Dotinga is a freelance medical and science journalist based in San Diego.
Disclosures
The study authors reported no conflicts of interest.
Baqai reported no conflicts of interest.
Primary Source
JAMA Ophthalmology
Source Reference: Huang P-C, et al “Epidermal growth factor receptor inhibitors for lung cancer and the risk of keratitis” JAMA Ophthalmol 2024; DOI: 10.1001/jamaophthalmol.2023.6089.
>>> Read full article>>>
Copyright for syndicated content belongs to the linked Source : MedPageToday – https://www.medpagetoday.com/ophthalmology/generalophthalmology/108249


{kind=link}